2021 ASCO年中进展:阑尾癌的多样性及治疗选择 |
您所在的位置:网站首页 › 杯状细胞和粘液腺可以切除吗 › 2021 ASCO年中进展:阑尾癌的多样性及治疗选择 |
2021 ASCO年中进展:阑尾癌的多样性及治疗选择
|
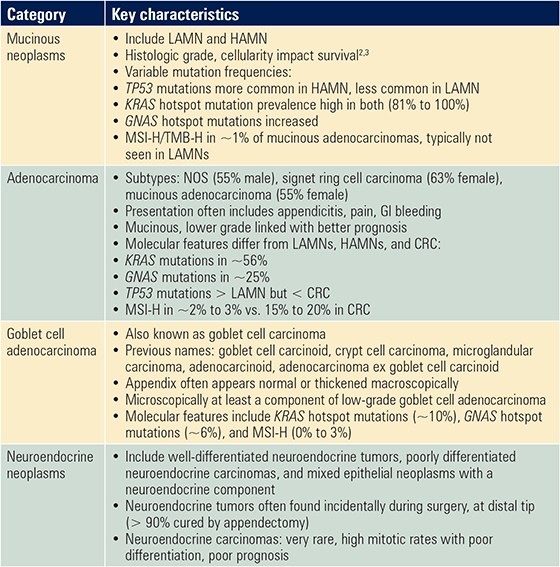
纪念斯隆凯特琳癌症中心的Jaclyn F. Hechtman教授在会议开始首先根据世界卫生组织的分类对阑尾肿瘤进行了全面概述 [1] ,包括阑尾癌的组织学和分子特征。表1总结了阑尾癌的主要特征 [2,3] 。 表1. 阑尾癌的特点总结
Abbreviations: CRC, colorectal cancer; GI, gastrointestinal; HAMN, high-grade appendiceal mucinous neoplasm; LAMN, low-grade appendiceal mucinous neoplasm; NOS, not otherwise specified; MSI-H, high-level microsatellite instability; TMB-H, high tumor mutational burden. 阑尾癌的创新系统治疗方案 Bahary教授总结了阑尾癌的全身治疗方法。目前还没有阑尾癌的治疗指南。对于阑尾癌患者通常使用结肠癌的治疗方法,而Ⅲ/Ⅳ期杯状细胞腺癌患者通常接受辅助化疗。 Bahary教授指出,阑尾癌与结肠癌不同,需要新的治疗模式。目前,研究人员正在开发的新疗法采用多种方法,包括分子靶向治疗。GNAS在杯状细胞癌中表达相对较低,而在腹膜黏液腺癌和假黏液瘤中表达较高。与印戒细胞癌和结直肠癌相比,KRAS在假性黏液瘤、腹膜和黏液腺癌中更容易发生突变 [4] 。用黏液溶解疗法治疗可以减少保护肿瘤细胞的黏液数量,可能会增强药物的渗透力。经腹腔注射菠萝蛋白酶和n -乙酰半胱氨酸治疗后,患者的黏液明显减少 [5] 。一些试验也将研究对阑尾癌的免疫治疗和溶瘤病毒治疗(表2)。 表2. 纳入阑尾癌患者的临床试验 Abbreviations: GMCSF, granulocyte-macrophage colony-stimulating factor; IL-2, interleukin-2; NAC, N-acetylcysteine. 阑尾癌的独特手术方法
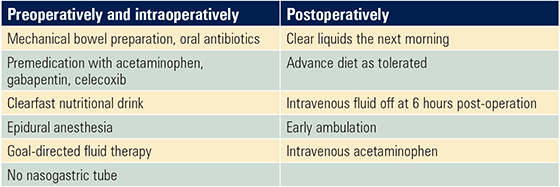
elya Melnitchouk 丹娜-法伯癌症研究所 丹娜-法伯癌症研究所的elya Melnitchouk教授对阑尾癌手术方法进行了概述。阑尾癌的手术治疗选择包括阑尾切除术、右结肠切除术,细胞减灭术加腹腔热化疗、加速康复外科加腹腔内热化疗以及姑息性手术。 Melnitchouk教授指出,对于阑尾低级别粘液性肿瘤或高级别粘液性肿瘤的患者,阑尾切除术通常是足够的。根据最近的文献报道 ,加速康复外科和腹腔内热化疗已经证明了一些益处(表3) [6,8] 。加速康复外科是可行的,应该更多地应用。 此外,加压腹腔气溶胶化疗是一种较新的治疗方法,已用于腹膜疾病患者,并可能是阑尾癌的另一种选择,有待进一步研究。 表3. 加速康复外科和腹腔内热化疗方案
总结 目前还没有阑尾癌的治疗指南。阑尾腺癌患者通常使用结肠癌治疗策略,而Ⅲ/Ⅳ期杯状细胞腺癌患者通常接受辅助化疗。包括分子靶向治疗在内的多种阑尾癌的新疗法正在开发中。 参考文献:(可上下滑动查看) 1. WHO Classification of Tumours Editorial Board. Digestive System Tumours: WHO Classification of Tumours (5th ed., Vol. 1). 2019. 2. Solomon D, Bekhor E, Leigh N, et al. Surveillance of low-grade appendiceal mucinous neoplasms with peritoneal metastases after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: Are 5 Years Enough? A Multisite Experience. Ann Surg Oncol. 2020;27:147-153. 3. Kyang LS, Alzahrani NA, Valle SJ, et al. Long-term survival outcomes of cytoreductive surgery and perioperative intraperitoneal chemotherapy: Single-institutional experience with 1225 cases. J Surg Oncol. 2019;120:794-802. 4. Ang CS, Shen JP, Hardy-Abeloos CJ, et al. Genomic Landscape of Appendiceal Neoplasms. JCO Precis Oncol. 2018;2:PO.17.00302. 5. Valle SJ, Akhter J, Mekkawy AH, et al. A novel treatment of bromelain and acetylcysteine (BromAc) in patients with peritoneal mucinous tumours: A phase I first in man study. Eur J Surg Oncol. 2021;47:115-122. 6. Lu PW, Fields AC, Shabat G, et al. Cytoreductive Surgery and HIPEC in an Enhanced Recovery After Surgery Program: A Feasibility Study. J Surg Res. 2020;247:59-65. 7. Webb C, Day R, Velazco CS, et al. Implementation of an enhanced recovery after surgery (eras) program is associated with improved outcomes in patients undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol. 2020;27:303-312. 8. Siddharthan R, Dewey E, Billingsley K, et al. Feasibility and benefits of an enhanced recovery after surgery protocol for patients undergoing cytoreductive surgery and heated intraperitoneal chemotherapy: A single institution experience. Am J Surg. 2020;219:1073-107. “肿瘤瞭望-消化时讯”读者专属微信群建好了,快快加入吧。扫描“肿瘤瞭望-消化时讯”小助手二维码(微信号: xhsx2021),回复“肿瘤瞭望-消化时讯读者”,ta会尽快拉您入群滴 ! 来源: 肿瘤瞭望-消化时讯 版权声明 凡署名原创的文章版权属“肿瘤瞭望-消化时讯”所有。欢迎个人转发分享。其他任何媒体、网站如需转载或引用本网版权所有之内容须在醒目位置处注明转自“肿瘤瞭望-消化时讯”返回搜狐,查看更多 |

【本文地址】