脑出血CT、MRI之争的终结者:GRE序列(T2*&SWI) |
您所在的位置:网站首页 › mri的t1和t2怎么看 › 脑出血CT、MRI之争的终结者:GRE序列(T2*&SWI) |
脑出血CT、MRI之争的终结者:GRE序列(T2*&SWI)
|
(点击可查看高清大图) 图2 比较大的出血
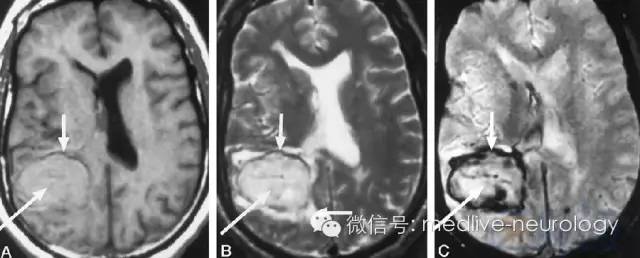
(点击可查看高清大图) 急性期 (1-3d) 图3
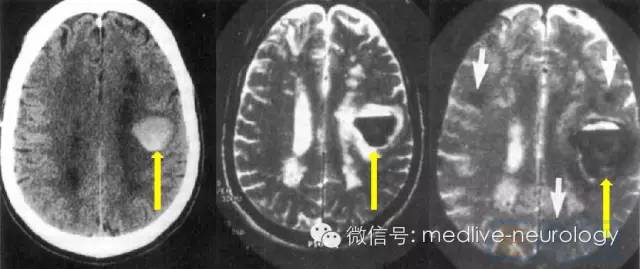
(点击可查看高清大图) 亚急性早期 (3-7d) 图4 (T1稍微不太典型哈)
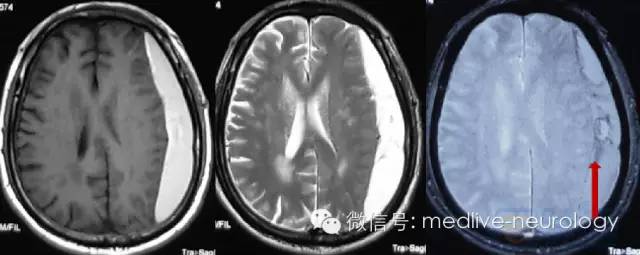
(点击可查看高清大图) 亚急性晚期(7-14d)(左硬膜下) 图5
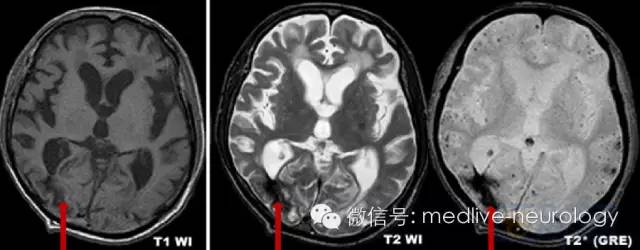
(点击可查看高清大图) 慢性期 (>14d) 图6
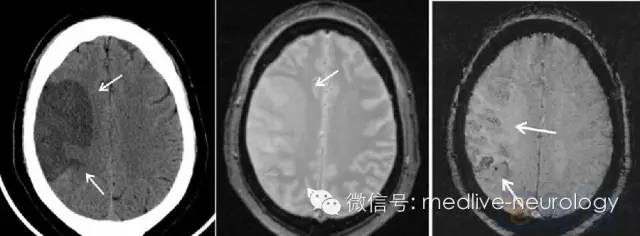
(点击可查看高清大图) 大家发现什么规律了吗?超急性期,各个研究相对一致,血肿中心出血比较新鲜,红细胞也是好的,氧合血红蛋白的氧还在;但血肿周边率先实现脱氧,顺磁性的脱氧血红蛋白就在T2*上造成了低信号,之后顺磁性物质(脱氧血红蛋白、正铁血红蛋白、含铁血黄素)越来越多,低信号的范围也就逐渐增加,但后续形态上确实不是特别规律,和血肿大小、有无脑脊液混合、有无再出血、演变过程等相关,就不要强求统一了。 但是不是有的童鞋还见到过SWI(susceptibility-weighted imaging,磁敏感加权成像),和T2*模样似乎差不多,但感觉也不完全一样,颇有双免傍地走,安能辨我是雄雌的赶脚。又是怎么一回事呢?下面先看两个图: 图7 脑梗死急性期周边渗血,最左边CT显示梗死病灶
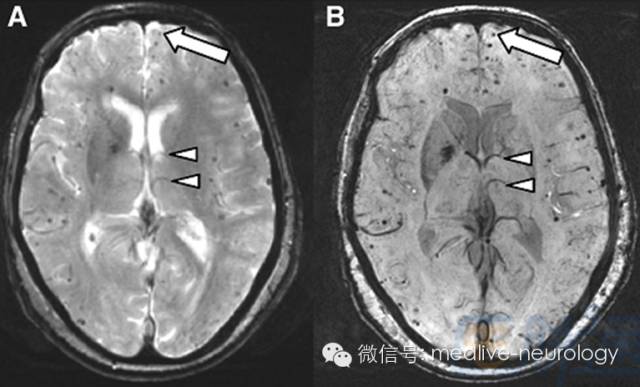
(点击可查看高清大图) 图8 近几年大热的微出血,大箭头为微出血,小三角为静脉。
(点击可查看高清大图) 这两个哪个是T2*,哪个是SWI呢?有没有觉得一个模糊点,一个清楚点?对了,那个锐利一些(最右边)的就是新生代SWI。虽然SWI问世并不是很晚,1997年就有人研究了。但在脑出血方面走了点弯路,一开始名字叫个拗口的基于脱氧血红蛋白的静脉核磁成像(MR venography with deoxyhemoglobin),去搞静脉成像。后来才浪子回头去琢磨出血。T2*和SWI两个关系很暧昧,都用的GRE序列,但SWI又经过了一系列复杂的成像过程和计算,玩弄些吓人的名词,什么magnitude, phase之类的,还有一堆公式,反正我是没弄明白怎么算出来的。总之,大家就当他们是远房亲戚好了,并且SWI是个青出于蓝的晚辈。显示出血里面这些顺磁性物质的低信号更突出,甚至有人还说它对于静脉、基底节铁沉积和出血看的太清楚了,会不会能力太强互相干扰呢?不过还好,后续的一系列研究证明SWI在卒中急性期出血优于T2*(图7)[7],并且检出微出血的能力也强于T2*(图8)[8]。但T2*已经抢先一步做过前瞻性的大型临床研究了,SWI在这方面就稍微欠缺了一点。不过小打小闹的研究证明SWI还是很优异的。回到图7,可以看出来即使是脑梗死早期细微的渗血,SWI也比经典的所谓的出血金标准CT和老前辈T2*要来的清晰。 参考文献: 1.Adams HP, Jr., Adams RJ, Brott T et al. Guidelines for the early management of patients with ischemic stroke: A scientific statement from the Stroke Council of the American Stroke Association. Stroke. 34(4), 1056-1083 (2003). 2.Kidwell CS, Chalela JA, Saver JL et al. Comparison of MRI and CT for detection of acute intracerebral hemorrhage. JAMA. 292(15), 1823-1830 (2004). 3.Fiebach JB, Schellinger PD, Gass A et al. Stroke magnetic resonance imaging is accurate in hyperacute intracerebral hemorrhage: a multicenter study on the validity of stroke imaging. Stroke. 35(2), 502-506 (2004). 4.Adams HP, Jr., del Zoppo G, Alberts MJ et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 115(20), e478-534 (2007). 5.Jauch EC, Saver JL, Adams HP, Jr. et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 44(3), 870-947 (2013). 6.Chavhan GB, Babyn PS, Thomas B, Shroff MM, Haacke EM. Principles, techniques, and applications of T2*-based MR imaging and its special applications. Radiographics. 29(5), 1433-1449 (2009). 7.Wycliffe ND, Choe J, Holshouser B, Oyoyo UE, Haacke EM, Kido DK. Reliability in detection of hemorrhage in acute stroke by a new three-dimensional gradient recalled echo susceptibility-weighted imaging technique compared to computed tomography: a retrospective study. J Magn Reson Imaging. 20(3), 372-377 (2004). 8.Cheng AL, Batool S, McCreary CR et al. Susceptibility-weighted imaging is more reliable than T2*-weighted gradient-recalled echo MRI for detecting microbleeds. Stroke. 44(10), 2782-2786 (2013). 版权声明【本微信所有转载文章出于传递更多信息之目的,且明确注明来源和作者,不希望被转载的媒体或个人可与我们联系,我们将立即进行删除处理】返回搜狐,查看更多 |

【本文地址】
今日新闻 |
推荐新闻 |